
what we do
Virtual Acute Care, LLC (V.A.C.) specializes in integration of real-life clinical expertise with advanced biosensor technology, Bluetooth-enabled devices, and continuous data monitoring and trending to deliver acute care to patients at home, skilled nursing facilities, and assisted living centers.
Our expertise is in design and development of innovative clinical workflows and care pathways that work for both patients and care providers. We partner with local medical experts and advanced biotechnology companies to deliver exceptional care wherever the patient happens to be.
A programmatic approach is BETTER
Most physicians and hospitals use an evidence-informed approach to care delivery which takes the research evidence and tries to apply them out of the context of the methods used to generate them. We use a truly evidence-based approach by creating programs with workflows that approximate the original clinical trial methodology, including the inclusion and exclusion criteria to select patients who will benefit most.
We make changes to the original methodology when we can demonstrate that such changes will result in more benefits, effectiveness, targeting, timeliness, efficiency, and reliability. We call this method of program redesign B.E.T.T.E.R. Quality Care (TM) and it’s the framework at the root of all our clinical programs and care pathways. Our programmatic approach means physicians, hospitals, and facilities do not order the technology, they order a program that uses the technology to deliver the desired outcomes.
our business is remote care delivery
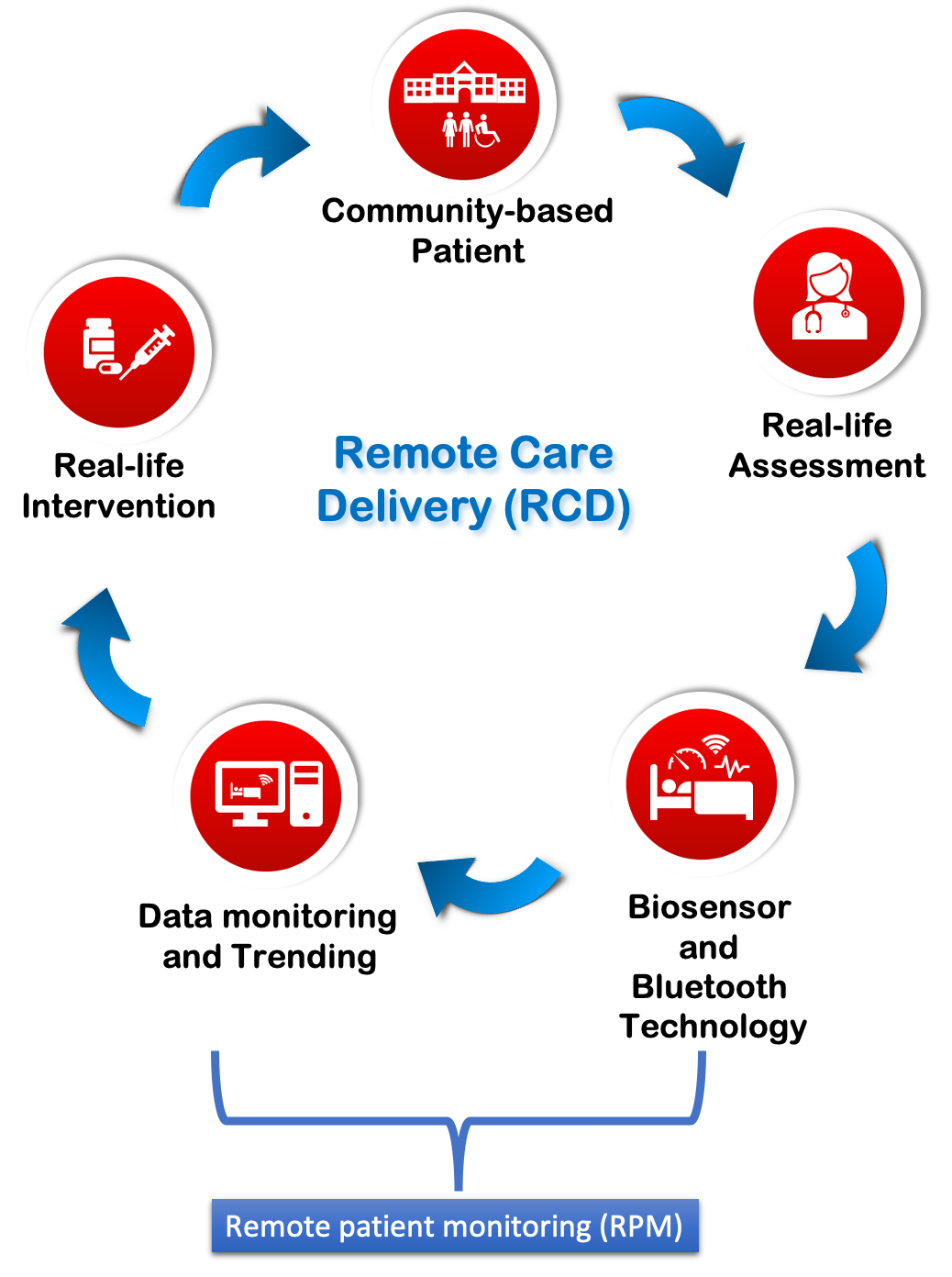
remote care delivery vs remote patient monitoring
Remote care delivery is a method of providing comprehensive care to a patient at a different location from the healthcare provider. Remote care delivery has been around for a long time. A nurse practitioner calling in a prescription for a patient at home or an on-call doctor at her house giving an order for treatment of a patient in the hospital are both examples of remote care delivery. More recently, eICUs have emerged as a sophisticated example of remote care delivery where doctors at a central location using advanced technology and telemonitoring are able to treat patients located in different ICUs at different hospitals.
Virtual Acute Care essentially does the same thing for outpatients using reliable data from biosensors and Bluetooth enabled devices which we combine with real life clinical assessment to develop and execute a treatment plan for patients at home and residents of skilled nursing facilities.
Virtual Acute Care is able to integrate vast amounts of data from remote patient monitoring because we have built a care delivery system that makes the data part of our daily workflow. This is no small accomplishment. Many physicians and practices can easily become overwhelmed by all the information from monitoring devices by different companies, calls from different labs, plus the information from nurses, home health agencies, and patients themselves (or their relatives). We avoid this by using a proprietary process improvement methodology for designing, developing, and implementing care delivery which conforms to the B.E.T.T.E.R. Quality Care framework.
CURRENT AREAS OF focus

snf programs

covid-19 units

transitional care
chronic disease
experience = opportunities + successes – failures
our 3-step virtual acute care process
Virtual Acute Care was conceived to allow mild to moderately symptomatic patients to be monitored at home instead of staying in an ED observation unit. The program has since evolved during the COVID-19 pandemic and is now focused on using innovative applications of technology coupled with real life care delivery using innovative care pathways to help preserve acute care hospital bed capacity by reducing unnecessary utilization by patients who can be safely treated as outpatients. Our programs all follow a similar 3-step process as that described below for the SNF program.
Patient Selection
One key to the SNF program’s success is appropriate patient selection. These tend to be patients with multiple chronic conditions who develop mild to moderate cardiopulmonary symptoms unrelated to COVID-19. These patients do not display high risk signs or symptoms on initial assessment but ED doctors worry about them because their chronic conditions can exacerbate later. These patients are usually kept in the observation unit as a safety precaution because they are not sick enough for admission and too sick to be sent home without close follow up. V.A.C was created to offer a third option which allows patients to be sent home or back to their skilled facility with hospital level monitoring and 24/7 cardiopulmonary care team coverage .
The V.A.C. program follows a three step process:
- Step 1-INITIATION : Face to face assessment by a care delivery team (CDT) with expertise in cardiopulmonary medicine and geriatric care medicine. The assessment includes a comprehensive review of the status of all chronic conditions using a multipoint evaluation tool coupled with thorough history and physical examination. Labs and point of care imaging studies (typically heart and lung ultrasound) are also obtained when indicated. A risk score is generated from the initial data set and used to create an individualized plan of care. High risk patients identified by the screening are immediately referred to the hospital for admission.
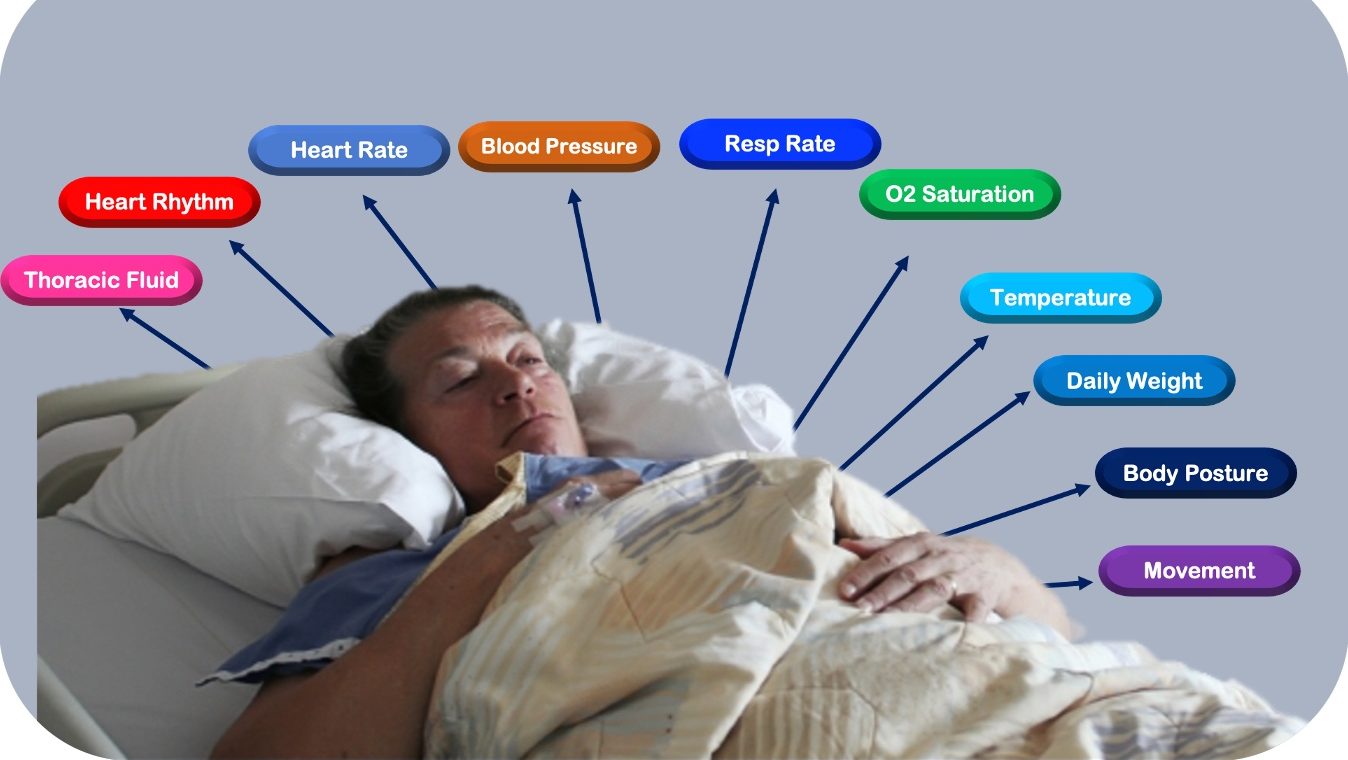
- Step 2-FACILITATION: Patients with mild to moderate risk are initiated on Virtual Acute Care (V.A.C.) program with remote monitoring system placement after appropriate consents are obtained. Monitoring is typically focused on key vital signs and clinical parameters with thoracic fluid index measurement included in those instances where heart failure is a major concern. Patients are typically monitored for 5-7 days. Team rounds are conducted every day by the CDT either in person or by using a pre-positioned telemedicine cart in patient’s room. The CDT tries to include the nursing team on rounds so everyone is on the same page. Rounds include discussions with the patient, review of data monitoring results, lab results, and any additional imaging studies. Changes to the treatment plan, including medication orders, are directly placed by the CDT into the facility EHR. A progress note is also placed in the EHR after rounds. If the patient is doing well on their daily risk assessment score then V.A.C. is continued, otherwise they will be sent to the hospital where the same CDT will admit and treat them there.
- Step 3-DISPOSITION: A final face to face assessment is performed at the end of the monitoring period to decide on disposition. Patients with resolved symptoms are discharged from V.A.C. program. Some discharged patients may need less intensive, Bluetooth based device monitoring for weight, blood pressure, and O2 saturations for chronic disease management. At any time during monitoring, a patient without the expected improvement or who has a worsening risk assessment score, is immediately referred to the hospital where the same CDT admits and seamlessly continues the patient’s care.
clinical expertise + Actionable monitoring Data = BETTER OUTCOMES
Virtual Acute Care’s programs leverage technology to extend the capability of frontline healthcare providers and improve the results of care. We collaborate with board certified medical specialists and highly trained advanced practice nurses who manage all clinical aspects of the programs, in collaboration with SNF medical directors and primary care providers. Such collaborative team-based care is critically important to the cost efficiency of our programs and prevents duplication of effort.
All monitoring data for the V.A.C. program is received and analyzed by FDA-cleared companies with secure advanced AI learning algorithms which are critical for individualized trend monitoring and alert generation. All patients in the V.A.C. program are covered 24/7 by by on-call locally available physicians.
![]() R
R